Knee Pain: Causes & Non-Surgical Treatments
Knee pain is one of the most common musculoskeletal complaints, affecting people of all ages and activity levels. The knee’s complex anatomy—bones, cartilage, ligaments, tendons, and bursae—means any structure can be the source of discomfort. Injuries, overuse, degenerative changes, and inflammatory conditions all play a role. A detailed history, physical exam, and appropriate imaging help pinpoint the cause and guide treatment. Many patients improve with conservative care (exercise, bracing, injections), but some ultimately require surgery to restore function and relieve pain.

What Are the Most Common Causes of Knee Pain?
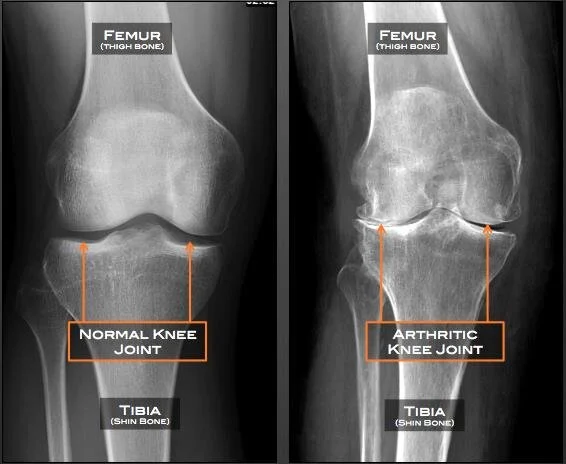
Osteoarthritis: Degeneration of joint cartilage leading to bone-on-bone contact, pain, and stiffness.
Patellofemoral Pain Syndrome: Maltracking of the kneecap causing pain under or around the patella.
Meniscal Tears: Damage to the shock-absorbing cartilage rings (menisci) from twisting injuries or degeneration.
Iliotibial (IT) Band Syndrome: Friction of the IT band on the outer femur, common in runners and cyclists.
Ligament Injuries: Sprains or tears of the ACL, PCL, MCL, or LCL causing instability and pain.
Bursitis & Tendinitis: Inflammation of the bursae or tendons from overuse or direct trauma.
Other Conditions: Gout, rheumatoid arthritis, Baker’s cysts, or referred pain from hip disorders.

Torn Lateral Meniscus
How Can I Treat Knee Pain Conservatively?
Exercise & Physical Therapy
Strengthen the quadriceps, hamstrings, hip abductors, and core to improve joint stability. Incorporate low-impact cardio (swimming, cycling) to maintain fitness without overloading the knee.Weight Management
Losing just 5–10% of body weight can substantially reduce knee-joint stress and ease osteoarthritis symptoms.Bracing & Orthotics
Unloader Braces shift force away from the diseased compartment.
Custom Orthotic Inserts correct foot biomechanics and improve knee alignment.
Activity Modification
Replace high-impact activities with low-impact options (water aerobics, elliptical) to protect the joint while staying active.

Physical therapy is crucial to the rehabilitation of most knee injuries
Which Injections Are Proven Effective?
Corticosteroid Injections
Provide short-term relief of inflammation and pain (typically 6–12 weeks). Repeat treatments should be spaced to minimize cartilage damage.Hyaluronic Acid (Viscosupplementation)
Aims to improve joint lubrication; results vary, and benefits tend to be modest.Platelet-Rich Plasma (PRP)
Uses concentrated growth factors from your own blood. Studies show modest pain and function improvement—especially at 6-month follow-up—though individual results vary.
Which Treatments Lack Proven Benefit?
Stem Cell Therapy (Mesenchymal Stem Cells)
Experimental: while early trials show promise, high variability and limited large-scale studies mean MSC injections remain unproven. Recommended only within clinical research.
| Learn more: Stem Cell Therapy for Joint Pain
Ultrasound-guided corticosteroid injection into knee joint for pain management

When Should I Consider Surgery for Knee Pain?
Meniscal Repair or Partial Meniscectomy
For acute, symptomatic tears unresponsive to 6 months of non-operative care or tears that mechanically block motion.Ligament Reconstruction
Indicated when ACL/PCL tears cause instability that limits daily activities or risks further joint damage.Osteotomy
Realigns bone to shift weight away from the damaged compartment; ideal for younger patients with unicompartmental arthritis.Total Knee Replacement
Recommended for end-stage osteoarthritis with severe pain, fixed deformity, or chronic inflammation not relieved by conservative measures.
Frequently Asked Questions (FAQ)
Q: How long does a corticosteroid injection last?
A: Relief typically lasts from 6 weeks up to 3 months, depending on disease severity and activity level.
Q: Is PRP better than hyaluronic acid?
A: PRP often shows greater pain reduction at 6 months, but individual results vary and insurance coverage may differ.
Q: When should I see a specialist?
A: If pain persists beyond 6–8 weeks despite home care, or if you experience locking, giving way, or severe swelling, schedule an evaluation.
Q: Can weight loss really help knee pain?
A: Yes—shedding just 5% of body weight can reduce knee-joint forces by up to 20%, markedly improving symptoms.
Q: Are stem cell injections safe?
A: Generally yes, since they use your own cells, but their efficacy is unproven—reserve for clinical trials.